Transcervical Vocal Fold Injection (In-Office)
Transcription
CHAPTER 1
I’m Seth Cohen, Associate Professor in the Department of Surgery in the Division of Head and Neck Surgery and Communications Sciences within the Duke Voice Care Center. I practice laryngology.
So anesthesia is really the key. So you can do this procedure and keeping the patient calm. So the way I do it, we use Avertin and tetracaine in the nose, to numb the nose, and then I'll use plain lidocaine without epinephrine. The way I usually like to do the procedure is through the cricothyroid membrane. So I will inject that plain lidocaine through the cricothyroid membrane, draw back and make sure I'm in the trachea by drawing back air. And then I’ll inject with the bevel pointed superiorly, so the lidocaine goes through the vocal folds and then falls and bathes the larynx. And then I'll use a little lidocaine with epinephrine to just numb the skin and the area over the cricothyroid membrane.
So anybody who needs augmentation of their vocal folds to help their problem, so unilateral vocal fold paralysis, unilateral vocal cord atrophy, or bilateral vocal cord atrophy, you can do both vocal folds at the same time in the office. It’s more convenient. It’s cheaper. You can get improvement the same day that you see the patient, and you can get some feedback, because the patient’s awake and talking to you while you do the injections. Obviously it depends on the patient tolerance, and it's a discussion that you have with the patient about options. I think anybody who has good anatomy, good tolerance, who's not too squeamish with needles, is a good candidate for the procedure.
When I first learned it, I guess I tried different ways of getting through the cartilage. But trying to go through the cartilage can be problematic, as the cartilage becomes ossified. I've tried various ways of numbing the patient including nebulizing lidocaine, and I find that just a little bit of lidocaine - I usually use one or two percent, 2 cc without epinephrine into the airway and then, at the most a half a cc of 1% with epinephrine in the skin gives the best anesthetic for me.
So certainly patient tolerance is one. Making sure you have good anesthesia. The anatomy is very important - so do you have good palpable landmarks? Do they have a really short neck where trying to get the angle to get the needle superiorly is important? I do put a bend on my needle, so that once you enter the cricothyroid membrane, you can then use the angle of the needle then to try and get superiorly to the vocal fold. It’s good to be facile with other options as well, such as a transcartilaginous approach or going through the thyrohyoid space, if for some reason you're having difficulty getting in through the cricothyroid membrane.
He's a cardiac patient and he had an idiopathic paralysis. So we got a CT scan, which you have to do to in those cases to make sure that there's not a lesion involving the vagus or recurrent laryngeal nerve. He did not. So hopefully, there’s a good chance this won't return, but he was incredibly hoarse. Very breathy, and you know when you have a vocal fold paralysis, you affect your ability to swallow potentially, your ability to have a good cough, your ability to talk, and because you can’t do a good Valsalva, your energy level goes down. He had good, palpable landmarks. We talked about what would be involved with the office injection. He thought he could tolerate it. So he was a good candidate for the procedure.
One thing I should mention too is you need a partner. The way I like to do it uses the flexibility of the laryngoscope, and then you're managing the needle with the collagen. You know, I had the patient sit upright, close their mouth, and breathe in slowly through their nose, and try and relax.
Just because of the anesthetic, I limit them not to eat or drink for 2 hours until all the sensation comes back in their larynx. But I do usually do let them talk, afterwards. I explain that the voice maybe worse before it gets better, because this is a temporizing measure, so I typically will over-inject with the collagen on purpose to get it to last as long as possible.
So for him, his vocal cord enclosure was pretty poor, so voice therapy really was not an option for him. Because it was idiopathic, and it was early in the onset, I would not proceed directly to a permanent laryngoplasty. So for him, I think the only other option was doing this in the operating room. Being on blood thinners and being a cardiac patient, there’s risks with general anesthesia, so I think overall, from a morbidity standpoint, this is certainly safer for the patient. And certainly I would be amenable to having that done in the office versus having to be NPO after midnight, go to the operating room, and then have to recover from anesthetic.
CHAPTER 2
So I’m just going to - this is just some lidocaine, okay? Yep. And we’re going to inject into the cricothyroid space with the bevel pointed superiorly, so the medicine will go through the vocal cords and then fall down and numb - numb the area from the inside, okay? You’re going to feel a pinch, and then you will cough for a few seconds. Just hold really still and don't bump my arm. I draw back until I get air, and then brace my left hand because he's going to cough and get that in as quickly as we can. [Patient coughs.] And there’s the cough, that’s mixing the lidocaine around everywhere. Yeah. And then this is just a bit more lidocaine that we’re just going to do in the skin, okay? And I always do the other part first so I don’t cause a huge bleb, and then have a hard time getting the lidocaine endolaryngeal because that’s where we really need the lidocaine. Okay, and while that’s working I’m going to get everything mixed up, okay?
CHAPTER 3
And she’s already sprayed your nose. And I'm just mixing it up with some injectable saline. Do you have a certain amount that you use? I do - 1.7. Sometimes I try and cheat and do a tiny bit less, so about 1.6 sometimes. But if you make it too thick, it’s hard to inject the Cymetra through the needle. So you can’t get rid of too much of the saline. And then, because this can clump sometimes, what I do is I’ve already pulled the syringe back from 2 to 3 mLs and banged it around a little bit.
CHAPTER 4
And then you want to get the air - get the saline up flush with this connector, and this is the most important part, is I have to get saline to the plunger, so it doesn’t clump. So I do it really fast and keep the pressure on there. And now I’ve got plenty of saline down here, and then a few more little bangs to distribute that and then back and forth quickly, and now we don’t have any clumps. Now I just have to get the air out. So back and forth and then let the air come back into the 3 cc syringe, and then you just do that a few times, and then eventually all the air will come out. Okay, so now we have no more air, so we are ready to go.
CHAPTER 5
And then I take one of these 1.5-inch, 23-gauge needles. And make sure my Cymetra will go through. So I’m getting it out the end, and because I like to go through the cricothyroid space, sometimes it’s harder to go through the cartilage, and I’m going to put a bend on this. Make sure it’s still running. And then the angle we’re going to try and do is go laterally through the cricothyroid space, and then we have to drop our hand down pretty quickly. And sometimes, people with short necks, it’s hard to get that angle to get secure enough. So I find that that bend helps a little bit. And then we’re going to put the camera in the opposite nose. And since we’re doing the right side, we’ll try and go in the left nose to have a good view. And you’re comfortable? Yep. Okay. Do you want something behind your head? I’m all right. Okay. Just breathe. And we can see the blood from my injection. And we’ll just take a quick picture before. And say, "E." Say "Eee." "Eee." Try and hold that one more time. Can you swallow for me sir? Excellent. Good, and "Eee". "Eee." Try and hold it, "Eee." "Eee."
CHAPTER 6
Okay. All right, so nice, easy breathing now, okay? I’m going to see if I can slide in here. Okay. So I’m getting closer, but I’m still too inferior. Almost there. That's right, hang tight, you’re doing great.
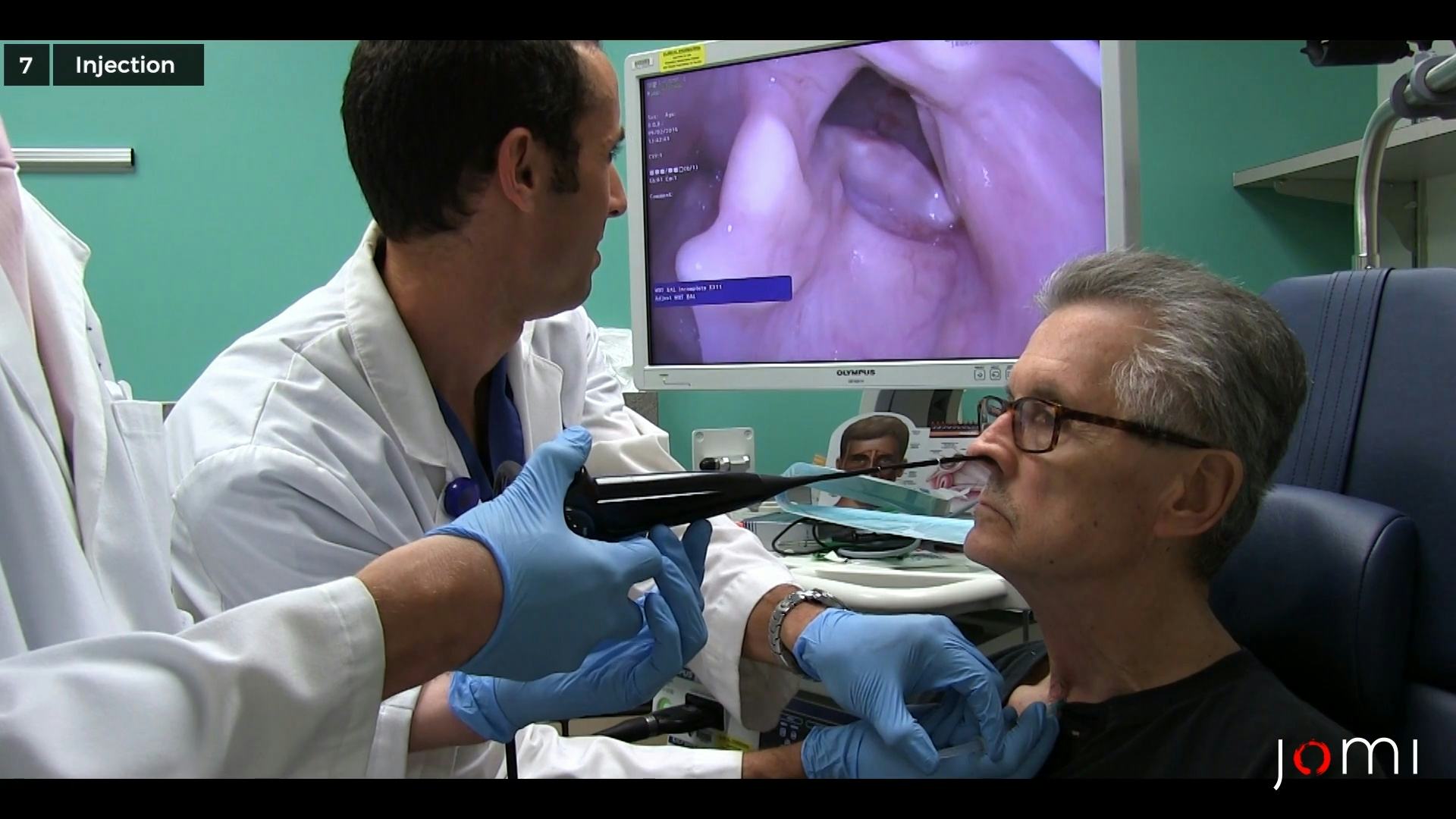
CHAPTER 7
All right so I’m right in the vocal cord now. Hold really still. Okay. It’s getting really fat, and then we’ll take a picture again. And say, "Eee." "Eee." One more time, hold it out, "Eee." "Eee." Okay. All done.