Minimally Invasive Open Preperitoneal Inguinal Hernia Repair
100913 views
Procedure Outline
Table of Contents
- Sedation is given at the beginning of the case while the patient is in the operating room
- 0.5% Marcaine + 1% lidocaine with epinephrine infiltrated into skin and subcutaneous tissues at beginning of case
- Ilioinguinal block given at beginning of case with same local anesthetic
- Local anesthetic also infiltrated before each tissue plane opened
- 10 cc of the local mix is is placed into the preperitoneal space at the initiation of the preperitoneal dissection in order to minimize the sedation used
- Patient is placed in supine position
- Ensure that all bony prominences are padded
- Transverse incision marked 1 cm above the halfway point on the line drawn between ipsilateral pubic tubercle and anterior superior iliac spine. The incision is 1/3rd lateral and 2/3rds medial (3.0 - 4.5 cm)
- Incision made in the skin and subcutaneous tissues
- Local infiltrated under external oblique
- External oblique opened along axis of muscle fibers
- Local anesthetic infiltrated into junction of internal oblique and rectus sheath
- Internal oblique opened in muscle-splitting fashion to expose transversalis fascia
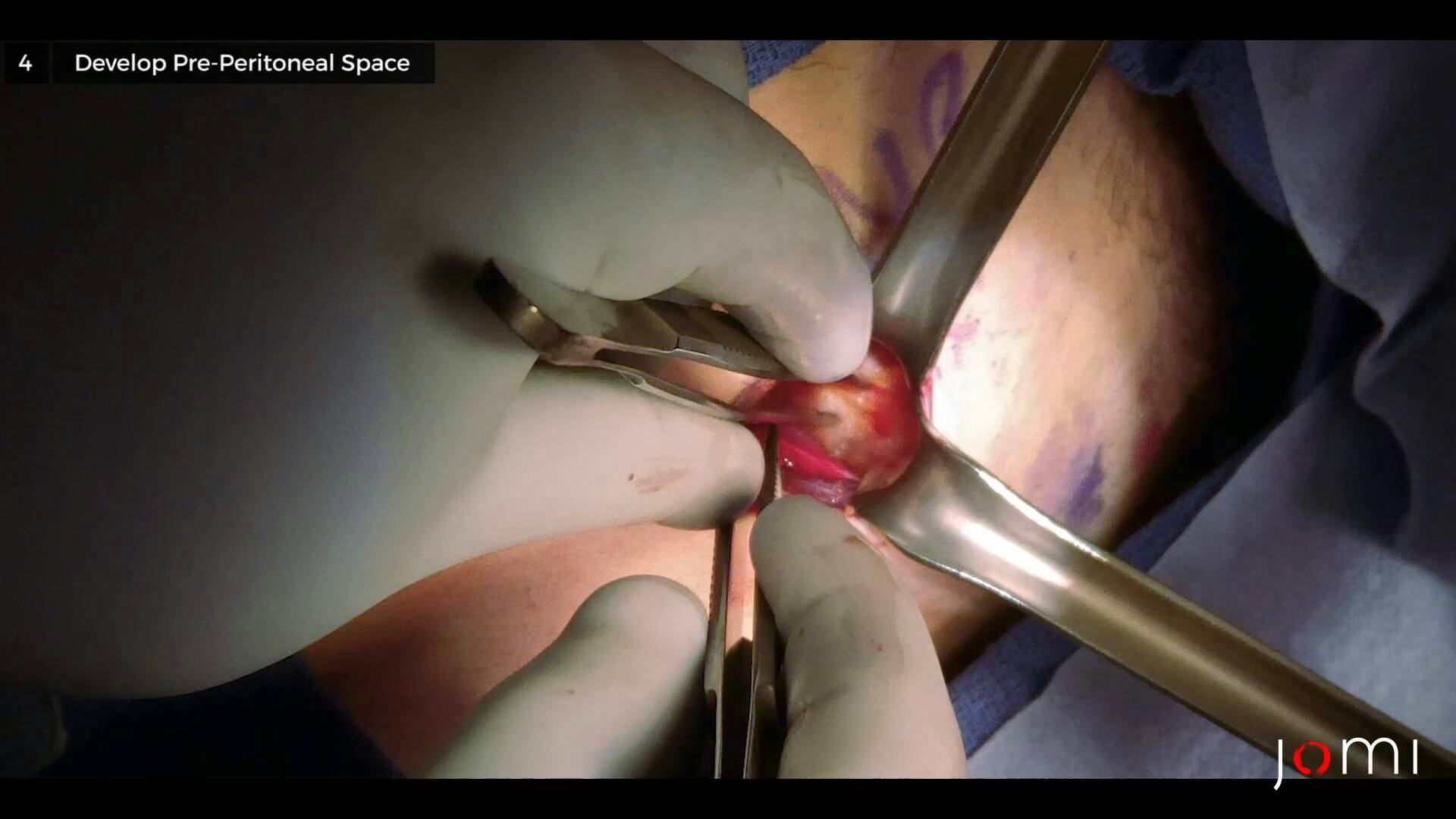
- Transversalis fascia opened to expose preperitoneal space, taking care not to injure inferior epigastric vessels
- Peritoneum separated from anterior abdominal wall via blunt dissection. Typically the dissection is performed from lateral to medial
- Hernia sac dissected free of attachments from internal ring, past bifurcation of spermatic cord where vas deferens deflects medially
- Peritoneum slowly teased away from the transversalis fascia along Hasselbach’s triangle to address direct hernia component
- Development of preperitoneal space below Cooper’s ligament
- Placement of Ventrio ST mesh within preperitoneal space to address indirect, direct and femoral spaces, with no suture anchors placed
- 3-0 Vicryl used to re-approximate external oblique fascia
- 3-0 Vicryl used to close Scarpa’s fascia
- 4-0 Vicryl as running suture used to close skin
- Oral acetaminophen and ibuprofen for pain control
- Toradol 30mg IV usually given in the OR
- Patients are provided a prescription for vicodin if needed - Typically less than 50% usage
- Foll Activity restriction for 2 weeks. Treadmill and exercise bike use as tolerated