Peroneal Tendon Debridement
29653 views
Procedure Outline
Table of Contents
- IV antibiotics were administered and a popliteal and saphenous nerve blocks were placed.
- Patient was placed in supine position.
- General Anesthesia was administered and a tourniquet was placed on left upper extremity.
- The patient was then turned onto a lateral position and a beanbag (deflated with a vacuum) held the patient in this position.
- Standard sterile prep and draping of the left lower extremity was done.
- The peroneal nerve of the left leg was padded and the medial prominences of the lower extremities were padded with foam.
- A curvilinear incision was marked out over the posterolateral aspect of the fibula following the path of the peroneous brevis tendon.
- The foot was then exsanguinated using an Esmarch bandage, and the tourniquet was inflated.
- The incision was made from approximately 4 cm above the distal tip of the patient's medial malleolus to the level of the tip of the medial malleolus.
- Great care was taken not to injure the peroneal nerve. Once it was identified, it was swept inferiorly and posteriorly.
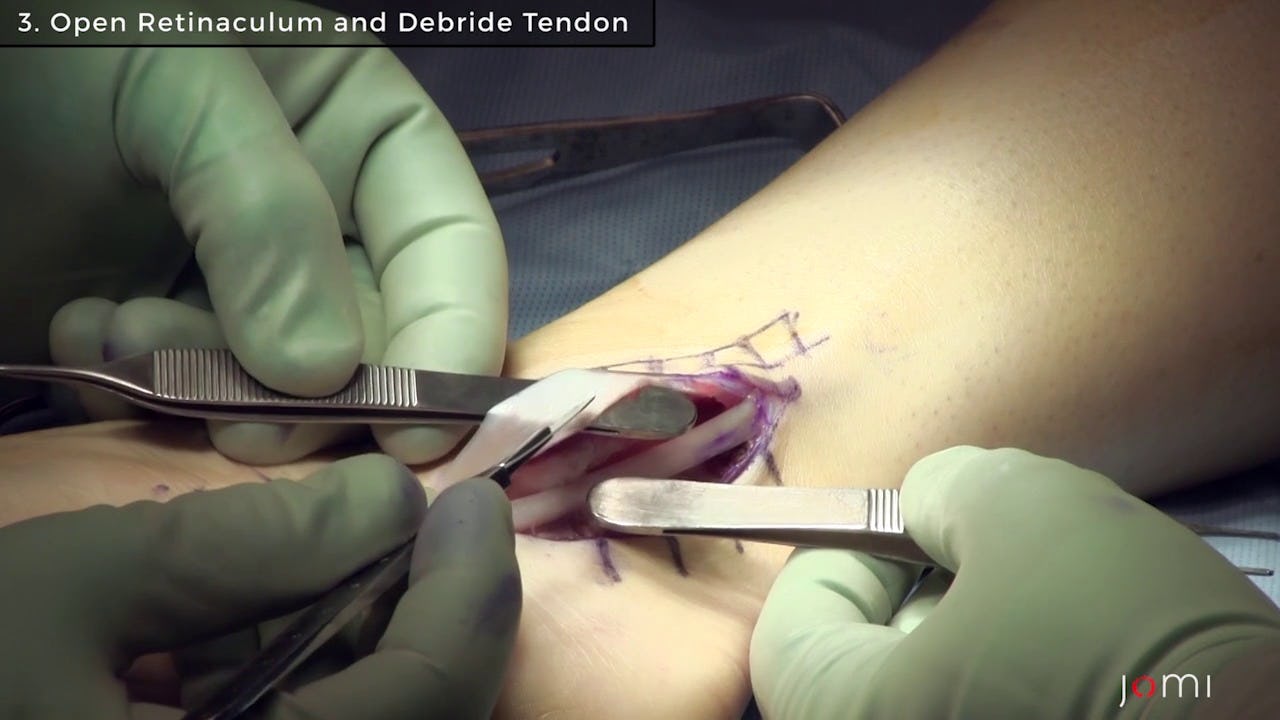
- Soft tissue dissection was performed down to the retinaculum of the peroneal tendons.
- Sharp dissection was used to open this retinaculum. Within the retinaculum there was a significant amount of inflamed tenosynovium surrounding the peroneal tendons. Also a low-lying muscle belly of the peroneus brevis was present. This extended down through the retinaculum to the level of the inferior fibular groove.
- The tenosynovium was debrided back and the low-lying muscle belly was resected to a level above the start of the fibular groove.
- Peroneus Quartus was also debrided.
- Inspection of the fibular groove showed that it was shallow and almost flat. The tendons showed good stability within the groove even with dorsiflexion and eversion.
- Three woven sutures were then passed through the bone to fashion the retinaculum back to the posterior portion of the fibula. This was then oversewn with 2-0 Vicryl sutures.
- The peroneal tendon excursion was tested in the reconstructed groove and retinaculum. There was no catching. Free excursion of the tendons was noted.
- The wound was thoroughly irrigated and the skin was then closed in layered fashion.
- The wound was then cleaned and dressed using Xeroform, fluffs, and Webril.
- A posterior short leg plaster splint was applied in neutral position.
- The tourniquet was released and the splint held in place until its hardening.
After emergence from General Anesthesia, the patient was extubated by the Anesthetist and taken to the Post Anesthesia Recovery Unit.