Resection of a Sphenoid Wing Meningioma
Charite Hospital Berlin
Transcription
Hello, my name is Marcus Czebanka. Today, we gonna resect a left-sided sphenoid wing meningioma. You can see the images over here. It's a 43-year old patient that actually complained about short episodes of speech arrest as well as of aura-like symptoms that have been going on for almost 4 weeks. Because of this reason, the patient received an MRI, and the - the results you can see over there.
In order to resect this kind of tumor you need five steps. The first step obviously is the approach and the craniotomy. In order to reach this tumor, we gonna use a pterional approach. The second step would be identification of the tumor and devascularization of the tumor. The third step is preparation of the tumor margins and separation of the tumor margins from the surrounding brain and especially from the internal carotid artery that's very closely associated in this case. The fourth step then is removal of the tumor, and the fifth step will be closing.
CHAPTER 1
So the first step now is skin incision for pterional craniotomy. B-pole. B-pole. We always use a combined skin muscle flap for this kind of approach. So we are not gonna separate the muscle over a large area from the skin. Okay, now we place the burr hole. Dissector. So we always place it underneath the temporal muscle. We just use one burr hole. Okay, now we’ve done the cuts for the craniotomy, and we just have a remaining part on the sphenoid bone underneath - and this we gonna drill. Now we gonna flip the flap. Flip the flap, that’s a good way of saying it. Now we are gonna flip the flap… B-pole. B-pole. Pardon me? Yeah, it doesn’t matter. It’s bleeding from the meningioma probably.
CHAPTER 2
Now we have finished the craniotomy. We have the extension to the temporal - temporal bone, and we also did resect part of the sphenoid - sphenoid wing. So now we are ready to go, and I think after draping we can - we can switch to the microscope. B-pole. See, I’m annoyed that it’s always oozing from down here. So it’s always - there’s always some bleeding from here. So I have to get rid of this.
So now we open the dura after we get hemostasis. So when we incise the dura, we always watch the tip of the scissors - that we make sure we don’t run into the brain. Okay. B-pole. B-pole. There we go. There’s the tumor already. Here you can see it. B-pole. Okay. So what we gonna do now is we’re gonna try to get some CSF. The optic nerve is down here. So we drain CSF now to get some more space. For this purpose, I am opening now the optic cistern. Okay, so down here is the optic nerve. That gives you good control of the medial aspect of the tumor. There you go.
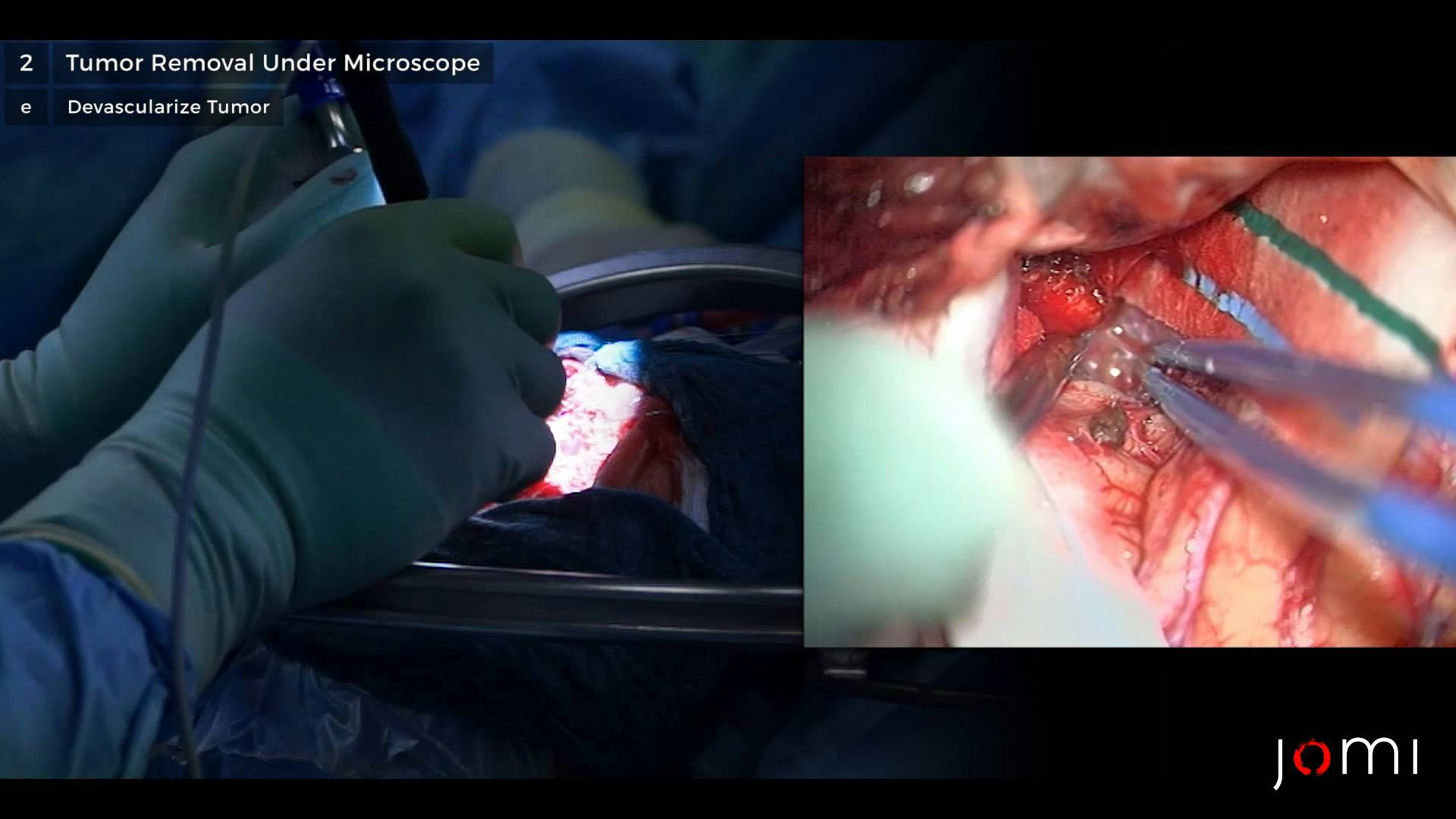
So now we are going to devascularize the tumor. B-pole. There you go. B-pole. So at the moment, I am having trouble getting a clear border between the tumor and the brain. B-pole. Now I’ve found the - now I’ve finally found the - the clear tumor border. Down here we can see the carotid artery. That’s the large bl - bla - brain supplying artery.
And I think now, we’ve made some progress. Okay. See that was all. I wasn’t able to find a good entry zone into the - for the border of the tumor and the brain. Now since we’ve found it, it’s getting much easier. Okay, this we’ll take care of later. B-pole. See now I’m approaching the circumferential preparation of the tumor borders. So once we have this posterior part, I think we should be all set to take it out. Here the tumor is still sticking to the dura, so I’m trying to re - go through here, and then we should be able to remove it en bloc. And the most safe part to remove definitely is the - the temporal polar part of the tumor. So that’s what I chose as the first part that I’m gonna resect. So this is gonna be the second part. B-pole. So that’s the blood supply of the dura. This - this you should coagulate. So that was - that was basically it.
Okay, just to show - okay here again, we have the optic nerve, and right next to it, we have the cari - internal carotid artery. And down here, you can see the oculomotor nerve, but this - everything’s okay. We have some arachnoid on it, so there should be - there - there should not be any problem with these structures. Just to make sure we don’t have any remnants of the tumor. That would be a pity. Okay, here you can see where the tumor was originating from. This we cannot resect. Therefore, we coagulated. If I ever find the - to get a Simpson grade 2 resection. Okay. So now we start closing the dura. We hope that it will close sufficiently. Sometimes the dura shrinks during surgery. Then we have trouble closing it. Okay.
CHAPTER 3
Is it okay? Okay. This we could do. That would be perfect - to discuss this surgery with a resident. Yeah, let’s do this. Oh, okay. So this procedure overall went very well. We could resect the tumor without any problems. The surgery was quick, and it was without any complications. In the beginning of the surgery, when I tried to do step number three, which is separation of the tumor margins from the surrounding brain, I had some difficulties because the tumor was very much attached to the surrounding brain, but finally we did get a good plane to really dissect the tumor from the brain. And therefore, the surgery overall went quite quickly without any problems.